THE
GOVERNMENT'S DRUGS POLICY: FOLLOW-UP
Submission
of Independent Drug Monitoring Unit
Matthew
J. Atha BSc MSc LL.B & Simon Davis DipHE (SocSci)
to
House
of Commons Home Affairs Select Committee
Foreword
F1
This memorandum represents some of the IDMU research findings
and issues raised in the course of legal casework since
our original submission to the committee enquiry dated
26-9-2001.
F2
IDMU is a small independent research consultancy specialising
in the study of illegal drug consumption patterns, prices
and effects. We are funded wholly via professional fees
earned in providing expert evidence for the criminal and
civil courts, with experience of over 1200 criminal cases
since 1991. The evidence mainly covers personal consumption
and drug valuations, but includes yields of cannabis cultivation
systems, effects of drugs (re criminal intent, driving
impairment etc.), and a range of other aspects, most notably
therapeutic uses of cannabis. Our mission is to provide
accurate, up to date and impartial information on drugs
to all parties to the debate over drugs policy. Other
than legal casework, we have provided consultancy for
GW Pharmaceuticals, the House of Lords enquiry, the Home
Office, Transport Research Laboratory, and Northamptonshire
Police.
1 Lambeth
Experiment
1.1
Fortuitously, IDMU has been monitoring the drug-using
behaviour of survey respondents resident in London who,
since May 2000, have completed questionnaires at the annual
"Legalise Cannabis" festival in Brixton. The
May 2000 data provides baseline figures, June 2001 coincided
with the start of the "experiment" where cannabis
use became effectively tolerated by the police, and May
2002 was a year into the experiment by which time any
consequences of the policy should have started to take
effect.
1.2
The preliminary results of this ongoing study show that
average monthly cannabis usage, purchase and spending
in 2002 had declined slightly, as had the average rating
of cannabis by users. Retail prices paid by Lambeth respondents
showed a slight, but non-significant increase. Cooperative
or commercial purchases were less frequent, with a higher
proportion used by the buyer him/herself. The average
age of initiation to cannabis use increased significantly,
supporting my long-held view that usage would increase
more among the older generation than among teenagers were
the law to be relaxed further, also reflected in the older
average age of the respondents.
|
Lambeth
Experiment - Preliminary Data
|
|
Indicator
|
Year
|
| |
2000
|
2001
|
2002
|
|
Base (no of respondents)
|
338
|
267
|
264
|
|
Response Rate
|
58%
|
70%
|
76%
|
|
Average Age
|
27.23
|
26.81
|
29.01
|
|
Reefers per day (weekdays)
|
5.87
|
5.56
|
4.63
|
|
Reefers per day (weekends)
|
10.66
|
9.6
|
7.31
|
|
Cannabis Used per Month
|
31.73g
|
38.87g
|
27.25g
|
|
Cannabis purchase per month
|
41.18g
|
57.68g
|
31.58g
|
|
Avg % personal use
|
77%
|
67%
|
86%
|
|
Monthly Cannabis Spending
|
£ 67.58
|
£ 73.11
|
£ 74.99
|
|
Cannabis Rating (0-10)
|
8.51
|
8.48
|
8.29
|
|
Soap-Bar Resin 1/8oz price
|
£ 12.86
|
£ 12.36
|
£ 12.91
|
|
Resin oz price
|
£ 69.93
|
£ 61.22
|
£ 65.68
|
|
Resin 9oz
|
£ 446.11
|
£ 393.64
|
£ 298.75
|
|
Skunk Herbal 1/8oz
|
£ 21.07
|
£ 20.52
|
£ 20.69
|
|
Skunk oz
|
£ 121.61
|
£ 119.85
|
£ 125.48
|
|
Skunk 9oz
|
£ 740.00
|
£ 640.91
|
£ 883.33
|
|
Age 1st Use of Cannabis
|
15.61
|
15.26
|
16.12
|
1.3
The preliminary conclusions to be drawn are that the Lambeth
experiment appears to have made little difference to the
consumption of cannabis users, but that any effect would
appear at this stage to be moderating influence on cannabis
usage rather than encouragement. Fears of increased cannabis
usage as a result of the experiment would thus appear
unfounded.
2. Drug
Prices
2.1
Cannabis: Prices of cannabis resin are continuing
to fall around the country as a whole, although there
are signs of the price of cannabis resin "bottoming
out", with the typical price now £10 per 1/8oz rather
than £15 in the mid 1990s, and a 9oz bar being sold for
£250-£400 rather than £600-£800 in 1994. Skunk (domestically
produced) cannabis prices appear relatively stable, with
the typical price ranging from £15-£25 per 1/8oz, and
ounces from £100-£160. Imported cannabis bush remains
rare, although has been encountered more often in IDMU
Criminal cases over the past 12 months, with these prices
increasing slightly. More respondents are reporting "exotic"
cannabis resin varieties such as moroccan "pollen".
2.2
Stimulants: Purities of amphetamine appear to have
returned to the levels seen in the late 1990s, gram prices
remain relatively stable within a range of £5 to £10,
although "ounce" prices appear to have increased
from £50-£80 to £70-£100 over the past two years. There
is still no evidence of any significant levels of methamphetamine
use (crystal meth, crank, ice etc) in the UK, despite
an epidemic in the USA. There are isolated seizures, mainly
in tablet form or powder sold as amphetamine sulphate.
Sensationalist publicity for methylamphetamine should
be avoided at all costs, lest it create a demand which
does not currently exist. The precursors used to manufacture
methamphet include over the counter medications and household
cleaning materials, thus no control on the availability
or tracking of precursor chemicals would be practicable
were usage of this drug to become commonplace.
2.3
Cocaine prices have remained stable within a range of
£40-£60 per gram, and £500-£1200 per ounce. Purities are
stable or rising. Crack prices again remain relatively
stable, but highlyvariable, with rocks of different sizes
available in different price bands.
2.4
Ecstasy prices are continuing a dramatic fall from £10-£15
per tab in 1994, down to £3-£5 per tab in 2002, with similar
falls at wholesale levels where prices of £1 or less per
tab are now common. Fewer "bogus" tablets are
being encountered, due to increased availability and use
of DIY pill-testing kits, most tablets sold as Ecstasy
contain 50-100mg MDMA.
2.5
Heroin prices are in long term decline. A "tenner
bag" may still cost £10, but whereas in 1994 it might
contain 80-100mg, these days they contain 100-250mg, and
£5 bags of around 100mg are increasingly common. Gram
prices vary across the country in a range of £30-£80,
ounces £500-£1000.
2.6
The Court of Appeal held in R-v-Edwards [2001]
that evidence in court by police officers or defence experts
as to drug consumption and prices would be ruled inadmissible
hearsay unless supported by statistical or scientific
evidence. In many cases prosecutions are undermined by
excessive valuations of drugs by police officers, many
of whom display a woeful ignorance of the drugs market
(e.g. claiming cannabis or cannabis resin is sold by the
gram), and who quote prices which those drug users among
the jury (statistically around 3-4 jury members will have
used cannabis or other drugs at least once, and 1-2 members
may be regular users familiar with current prices).
3 Drug
Prevalence (among drug users as a whole)
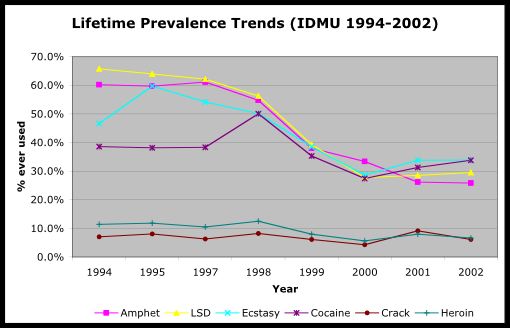
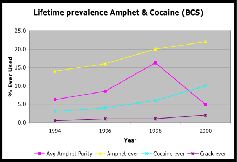
3.1
The prevalence of use of other controlled drugs among
users as a whole has declined since our 1994 survey, however
regular use of cocaine and crack has increased (the apparent
decrease in 2000 due to a survey design flaw which left
such questions to the end of a long and complicated survey,
causing a much higher proportion of incomplete questionnaires).
The decline in usage of other controlled drugs may reflect
increasing social acceptability of cannabis and use by
a wider segment of the population, not restricted to pre-existing
"drug subcultures" where use of different drugs
is tolerated.
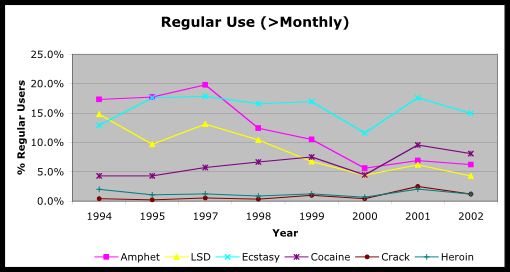
3.2
It would appear that the popularity of ecstasy has passed
its peak, with fewer users reporting regular use, despite
the dramatic fall in price. Whether this reflects a decline
in the dance culture, maturation out by the first waves
of ecstasy users, or increasing concerns about the long-term
mental health risks of ecstasy use remains an open question.
3.3
It is clear that with drugs other than cannabis, experimental
and occasional use remains the norm, with a very small
proportion using daily. The proportion of daily users
to lifetime, or regular, users is highest for heroin and
crack cocaine. However even with these "hard"
drugs, the majority who try them, or use occasionally,
do not become dependent.
4. Supply-side
Interventions - Operation Pirate
4.1
Operation Pirate led to the discovery in late 1998 of
the largest illicit drugs laboratory operation ever uncovered
on mainland Britain which saw 10 men sentenced for a total
of over 40 years for being part of a multi-million pound
amphetamine production conspiracy1
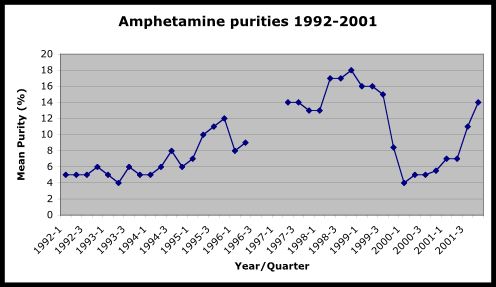
4.2
While usage of amphetamine by young people had been increasing
throughout the 1990s, with 8% of 16-29 year olds using
the drug in 1998, by 2000 that figure had fallen to 5%,
and the average purity had fallen from 16% to 5%, before
returning to pre-operation levels towards the end of 2001.
1
http://www.nationalcrimesquad.police.uk/Hot_off_the_press/info/106_record_jail_terms.html
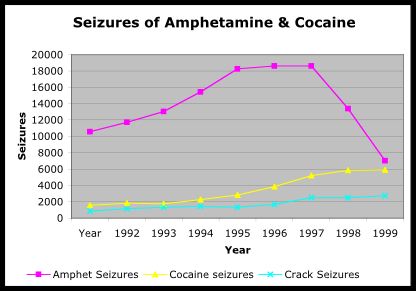
4.3
Prosecutions and seizures for amphetamine also fell sharply,
with the total number of amphetamine seizures falling
from over 18600 in 1998 to just over 7000 in 2000. A major
victory in the War on Drugs · or was it?
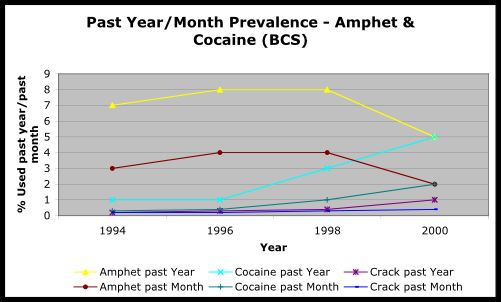
4.4
Britain"s "speed" users were suddenly left
without amphetamine to satisfy their cravings, at the
same time as record amounts of cocaine and crack were
entering the UK. Consequently although use in the past
year and past month of amphetamine halved between the
1998 and 2000 British Crime Surveys, usage of cocaine
and crack had doubled, such that by 2000 an equal number
had used amphetamine and cocaine in the previous 12 months.
4.5
The implications of this finding for supply-side control
and interdiction policies are gloomy. The most successful
anti-drugs operation in recent UK history merely resulted
in a high proportion of amphetamine users switching to
cocaine, and possibly also crack. One reason the UK never
experienced the US "crack" epidemic of the late
1980s and early 1990s, and for the relatively low prevalence
of cocaine usage, has been the wide availability of amphetamine,
which provides a similar effect for a longer duration
at a fraction of the cost.
4.6
The argument for "legalising" amphetamine is
undone by the propensity of the drug to cause aggression
and violence if used to excess, as well as physical health
risks associated with all stimulants. Thus an unrestricted
retail market would have adverse consequences for public
order and safety. Nonetheless, a form of controlled availability
- e.g. re a smart card for registered users specifying
a maximum daily or weekly "ration"/dose, or
prescription by GPs of dexamphetamine tablets or linctus
(to prevent injection) - might represent an alternative
method of "maintenance" treatment for individuals
with cocaine or crack dependency problems.
5. Medicinal
Necessity (Cannabis)
5.1
I am possibly the busiest court expert in this field,
having been involved as an expert in over 150 court cases.
Where a defence of medical necessity (duress of circumstances)
is put before a jury and supported by credible medical
evidence of a relevant condition, the jury almost always
acquits.
5.2
The principle of medical necessity in such cases has been
approved by the Court of Appeal in the case of Lockwood
[2002] · ironically one of the few defendants to have
been convicted. The defence has successfully been used
by patients with multiple sclerosis, chronic pain, epilepsy,
irritable bowel disease, cancer chemotherapy, gout, arthritis,
asthma, stress, anxiety, depression and Opiate dependency,
among other conditions, with juries tending to give a
wide interpretation to what is meant by "serious
injury". Where the defence is a mere "smokescreen"
to avoid conviction of dealing cannabis to non-patients,
juries rightly continue to convict.
5.2
Nonetheless, the Crown Prosecution Service almost invariably
proceed to trial in such cases, rather than abandoning
the prosecution when a medicinal defence is presented.
Despite my advice to both the Lords and Commons enquiries,
there are as yet no national guidelines as to which conditions
could provide a reasonable defence to cannabis possession
and/or cultivation charges. Each case must be examined
on its individual merits, but all such decisions to prosecute,
or continue with a prosecution, should first be reviewed
by a medical expert or panel of experts with the power
to discontinue proceedings where there is clear merit
in the defence, before further public money is wasted
on a jury trial.
6.
Implications of Reclassification
6.1
In our original submission of September 2001 we drew attention
to the pros and cons of different approaches to drug policy.
Our view remains that reclassification represents mere
tinkering at the edges of policy reform, where a root
and branch change could bear real results.
6.2
Our concern is that reclassification may make little difference
to the problems (social and financial) which drugs cause
society, unless the changed status is reflected in police
attitudes. It is the criminal record acquired by the user
which causes most damage to his or her future prospects,
irrespective of the penalty which results from it.
6.3
I can envisage a situation where some police officers
or forces allege "intent to supply" on ever-smaller
quantities of drugs, to "improve" their compliance
with performance targets, or to give themselves additional
powers (e.g. s18 PACE search) following an arrest. This
trend appears increasingly evident already, particularly
in rural forces (where users may have to travel to buy
their drugs and consequently buy more for themselves when
they have the opportunity). I would estimate that somewhere
around 60% or more of persons convicted of drugs supply
offences plead guilty on the basis of social supply (to
partner or friends) yet are convicted, on their record,
as drug dealers, but pleading (despite protestations of
innocence) due to the fear of being found guilty and imprisoned
as a result.
6.4
There should be national guidelines issued to police forces
for the quantities of drugs which would:
(a)
involve no action (e.g. up to 30g cannabis or up to 15
flowering plants)
(b)
charged with possession only (30-100g cannabis, 15-50
plants)
(c)
charged with possession only, unless there is supporting
evidence of dealing (cash, packaging materials, scales,
wrapped deals, dealer lists or documentations) where "intent"
charges might be brought (100-250g cannabis, 50-100 plants)
(d)
where intent charges may reasonably proceed on the basis
of quantity alone (over 250g cannabis or 100+ plants)
(e)
The burden of proof would remain on the prosecution to
prove an "intent" charge, based (e.g.) on the
defendant"s ability to fund a claimed level of usage
without resorting to dealing drugs.
6.5
For other drugs, the equivalent thresholds could reasonably
be
|
Drug
|
No
action
|
Poss
only
|
Poss
unless intent
|
Intent
|
|
Amphet
|
0-7g
|
7-20g
|
20-50g
|
>50g
|
|
Ecstasy
|
1-10 tbs
|
10-50tbs
|
50-100tbs
|
>100 tbs
|
|
LSD
|
1-10 tbs
|
10-50tbs
|
50-100tbs
|
>100 tbs
|
|
Cocaine
|
0-2g
|
2-10g
|
7-30g
|
>30g
|
|
Heroin
|
0-1g
|
1-4g
|
5-14g
|
>14g
|
|
Crack
|
0-1g
|
1-2g
|
2-10g
|
>10g
|
6.6
In the longer term, a coherent control policy would involve
controlled availability of different drugs according to
their potential dangers to the individual user and to
society.
6.7
Cannabis could be treated in a similar manner to tobacco
or alcohol, although to reduce the present availability
to children I would consider members-only clubs to be
the most appropriate legal outlet.
6.8
Stimulant drugs should be rationed, to deter the user
from consuming excessively and creating social problems
as a result, with cocaine users encouraged to use amphetamine
as a marginally safer alternative.
6.9
Heroin should be made available to existing users (verified
by urinalysis) on prescription, in an injectable or smokeable
form (e.g. laced cigarettes), as a matter of urgency,
in order to undercut the illicit market and make a significant
impact on acquisitive crime, as well as helping to stabilise
the chaotic lifestyles associated with problem use.
|
Controlled
Availability?
|
|
Cannabis
|
Licensed
premises (coffee shops or members-only clubs), excise
duty
|
|
Tobacco
|
Licensed
premises, excise duty
|
|
Alcohol
|
Licensed
premises, excise duty
|
|
Amphetamine
|
Prescription
only or rationing (smart card)
|
|
Cocaine
|
Prescription
or rationing (smart card), low dose preparations
(e.g. coca leaf), alternative stimulants (maintenance)
|
|
Heroin
|
Prescription
or rationing (smart card), low dose preparations
(e.g. opium)
|
|
Ecstasy
|
Rationing
(smart-card) · develop safer but effective legal
alternatives
|
|
Crack
|
No
availability, users could prepare from cocaine "ration"
alternative stimulants
|
6.10
The financial argument for licensing of cannabis (or other
drugs) has never convincingly been aired. There is no
doubt that substantial funds would become available to
the Treasury as a result of excise duty, although the
dramatic fall in prices of cannabis and ecstasy in recent
shows the limitations of any fixed duty levels.
6.11
Already the UK is moving towards self-sufficiency in cannabis,
with nearly 50% of the market now involving domestically-produced
(indoor) material. However any moves to licence the sale
of any currently illegal drug would require secession
from, or renegotiation of, existing international treaties.
I note the move towards reclassification has been criticised
by members of the the UNDCP executive. However as these
represent the very people who have presided over the failures
of international drugs policy for the past 30+ years,
such criticism is an understandable response to proposals
which could overturn their world view, particularly where
alternative approaches (e.g. the Netherlands) have proven
successful in reducing both the level of drug use and
of drug-related harm.
Matthew
Atha - Director
Simon
Davis -Research Co-ordinator
6
March 2003