Anabolic
Steroid Usage, Prices & Effects
Matthew
J Atha BSc MSc LL.B
Director
- Independent Drug Monitoring Unit
1
Introduction
1.1
Anabolic steroids are a group of compounds which mimic
sex and growth hormones in the body. They are typically
used without prescription by athletes and bodybuilders
in order to build up muscle mass and reduce the fatigue
involved in training regimes. There are around 500 steroidal
substances identified in mammals, with 5 major groups
distinguished by physiological action, these are glucocorticoids,
mineralocorticoids, androgens, oestrogens and progestins[1]. The classical
sex steroid is testosterone, which has many derivatives,
all of which are to a greater or lesser extent effective
as androgens (masculinising) and anabolics (tissue-building),
without separation of these two discrete effects, with
the result that the class is known as anabolic-androgenic
steroids. These promote tissue growth by reducing the
breakdown of protein, particularly following exercise.
1.2
The effects of steroids on mood has long been recognised,
from Aristotle prior to 300BC noting the psychological
and behavioural aspects of maleness. In the 1800s, the
testes were demonstrated to contain substances which
maintained vitality, strength, energy and youthfulness,
and sex-hormones were used to treat mood and mental
disorders in the early part of this century, particular
melancholia and depression. However, more recent studies
have pointed to severe behavioural side effects, including
violent psychotic episodes, associated with the use
of anabolic-androgenic steroids in particular users.
1.3
IDMU deals only rarely with cases involving anaboic
steroids and related bodybuilding products, and only
a handful of drug users report lifetime steroid use
each year in our surveys.
1.4
Unlike most controlled drugs, the majority of steroids
appear on the market as pharmaceutical preparations,
in blister packs of tablets, glass ampoules for injection,
or multi-dose vials, labelled with brand-names and/or
contents. Such products can be either legitimate - manufactured
legally by pharmaceutical companies, mainly overseas
- or counterfeit, where the contents do not match the
description and often contain either different substances
or no active ingredients.
2
Consumption of steroids
2.1
There are a number of sources on the internet which
outline regimes (cycles) whereby steroids are taken
as part of a training regime over a period of 6-12 weeks,
gradually increasing then reducing the dose and then
coming off completely (e.g. to enter a competition).
These regimes commonly recommend dosages well in excess
of recommended levels, sometimes 4-8 times the pharmaceutical
dose[2].
2.2
The recommended route of administration for steroids
is an intramuscular injection, which delivers the drug
to the site of action and bypasses first-pass metabolism
in the liver, as would occur with oral tablets/capsules,
with an increased risk of liver damage as a result.
Clearly, any medically-unsupervised injection practice
carries with it the risk of blood-borne infections such
as hepatitis and HIV.
2.3
A number of studies have considered steroid usage and
their effects on behaviour, including the syndrome popularly
known as Ìroid-rage". Pope & Katz[3], in a study of 41 bodybuilders
and US Footballers using 10-100 times the medical doses
of steroids (15mg-600mg per day), found 12% reported
Ìmajor" psychiatric symptoms from Ìstacking"
different preparations. In a controlled study using
20 healthy non-athletic male volunteers with no prior
history of steroid use, Su et al[4]
measured placebo baseline, low dose methyltestosterone
(40mg), high dose methyltestosterone (240mg) and placebo.
In a single case report, Conacher et al[5]
cited the case history of a 32 year old Canadian bodybuilder
convicted or murdering his partner. He had been taking
steroids for 3 months before the incident, at about
6 times the medical dose (6x tablets dianabol per day
plus one ÌDeca" injection per week). Corrigan[6] reports on a male bodybuilder
22 yrs who violently murdered a woman after an 8 week
course of 50mg per week nandrolone (deca-durabolin,
organon), increased to 85mg (of a veterinary preparation)
for 3 weeks before the murder.
2.4
The dosage is complicated by the plethora of counterfeit
pharmaceutical steroids available on the market. Although
anabolic steroids are controlled drugs in the UK, USA
and other developed countries, there are a number of
countries throughout the world where these are still
manufactured legitimately. Illicit steroid products
will commonly mimic the appearance or packaging of legitimate
products, but will often contain either a different
dosage or different drug to that denoted on the label.
This phenomenon is well known among regular steroid
users, and there are a number of internet publications
(mostly subscription only) which provide information
on the content of the latest products, and warnings
about faulty or counterfeit tablets.
3
Steroid Consumption -IDMU Survey Data
3.1
IDMU drug user surveys have included questions about
steroid usage, prices and attitudes since 1999.
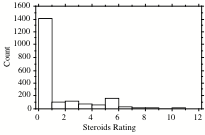
3.2
To date (Jan 2004), 10070 questionnaires have been returned
and analysed, from which only 157 (1.6%) respondents
have reported lifetime usage of steroids. The usage
pattern shows fewer regular (weekly/monthly) than daily
users, a similar ÌJ" shaped distribution to addictive
drugs such as heroin or crack (Table 1). Users generally
report higher ratings than non-users, a pattern common
with most illicit drugs.
|
Table
1 - Steroid Usage Data 1999-2003
|
|
Usage Level
|
n
|
%
|
Rating
|
|
Experimental
|
50
|
0.50%
|
3.19
|
|
Occasional
|
11
|
0.11%
|
6.71
|
|
Regular
|
7
|
0.07%
|
3.33
|
|
Daily
|
21
|
0.21%
|
3.80
|
|
Stopped Using
|
68
|
0.68%
|
1.55
|
|
Might Use
|
75
|
0.74%
|
2.13
|
|
Would Never Use
|
2596
|
25.8%
|
1.00
|
|
Other/Blank
|
7242
|
71.9%
|
1.12
|
|
Total Ever
|
157
|
1.57%
|
2.97
|
|
Saturation
|
67.7%
|
Overall
|
1.15
|
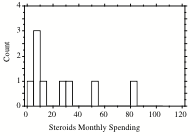
3.3
The drug has an overwhelmingly negative reputation among
drug users as a whole, with the average user-rating
of 1.15/10, among the lowest ratings for any drug, and
only 75 respondents (0.74%) who had not used the drug
being willing to try it. Average monthly spending (9x
respondents) was £23.57, with a maximum of £80 per month
(fig 1)
Fig
1 - Steroid Ratings & Monthly Spending 1999-2003
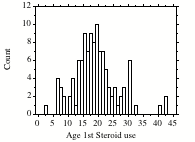
3.4
The age of initiation data, with a surprising 30% of
respondents reported first having used before age 15,
suggests that many respondents may have been using prescribed
steroids for medical conditions in childhood (fig 2),
although the majority started between ages 14 and 23,
consistent with use in connection with sporting activity.
Fig
2 - Age of Initation to Steroid Use
3.5
Summary: Usage of anabolic steroids is limited
to certain niche markets, and has little appeal to drug
users outside, bodybuilding/fitness, sports and Ìsecurity"
personnel. Whilst the number of regular users is very
small, they can use excessively - many times the therapeutic
dose. There is evidence of physical and psychological
dependence from prolonged use, risking a pattern of
violence and aggression commonly known as ÌRoid Rage".
4.
UK Steroid Prices
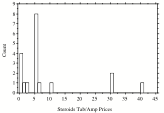
4.1
IDMU Survey Prices: The average reported prices
of steroid preparations in our suveys from 1999-2003
is shown in table 2, and the distribution of reported
prices between1999 and 2003 in fig 3 below. Note that
reports of steroid use or prices amongst users of illicit
drugs are very rare (19 reports from 10061 respondents),
and Ìtab/amp" prices do not distinguish between
different drug preparations and dosages.
|
Table
2 - UK Steroid Prices 1999-2003*
|
|
Type
|
Number
|
Price
|
|
Amp
|
6
|
£ 9.17
|
|
Tab
|
13
|
£ 7.99
|
|
Overall
|
19
|
£ 8.37
|
* Provisional 2003 dataset n=2040
Fig 3 - Steroid Price Distributions 1999-2003
4.2
Internet Prices: A range of steroid products
are available from internet retailers and wholesalers.
The prices depend on the type of steroid or brand, the
dosage, the quantity bought, and where manufactured
or sold.
4.3
A Google search for named steroid compounds revealed
several sites[7] offering online purchase
facilities, quoting prices in Euros and/or in US Dollars.
These have been converted to Sterling at approximate
prevailing exchange rates of €1.40=£1 and $1.60=£1.
Those entries denoted Ë(BNF)Ó are prices quoted in the
British National Formulary.
|
Table
3 - Online Prices of Anabolic Steroid Preparations
|
|
Trade Name and/or Drug
|
Preparation
|
Qty
|
Euros
|
Dollars
|
Sterling
|
Unit (£)
|
|
Anabol
(methanenedione)
|
tabs (5mg)
|
500
|
€ 220.00
|
|
£ 157.14
|
£ 0.31
|
|
Anabol
|
tabs (5mg)
|
50
|
|
$19.00
|
£ 11.88
|
£ 0.24
|
|
Anabol
|
tab (10mg)
|
50
|
|
$85.00
|
£ 53.13
|
£ 1.06
|
|
Anabol
5 mg.
|
tabs (5mg)
|
50
|
|
$45.00
|
£ 28.13
|
£ 0.56
|
|
Dianabol/Anabol
|
tab
|
1500
|
€ 479.00
|
|
£ 342.14
|
£ 0.23
|
|
Dianabol/Anabol
|
tabs (5mg)
|
100
|
€ 54.00
|
|
£ 38.57
|
£ 0.39
|
|
Methanenedione
|
tabs (50mg)
|
300
|
|
$450.00
|
£ 281.25
|
£ 0.94
|
|
Anadrol
- 50 (oxymetholone)
|
Tab
|
50
|
|
$250.00
|
£ 156.25
|
£ 3.13
|
|
Anadrol
- 50 (oxymetholone)
|
tab
|
200
|
|
$350.00
|
£ 218.75
|
£ 1.09
|
|
Anadrol
- Anapolone oxymetholone
|
tab (50mg)
|
20
|
€ 55.00
|
|
£ 39.29
|
£ 1.96
|
|
Anapolon
(oxyymetholone)
|
tabs (50mg)
|
100
|
|
$270.00
|
£ 168.75
|
£ 1.69
|
|
Boldabol
|
vial (200mg)
|
4
|
€ 375.00
|
|
£ 267.86
|
£ 66.96
|
|
Boldenone
Undeclynate
|
vial (200mg)
|
1
|
€ 125.00
|
|
£ 89.29
|
£ 89.29
|
|
Clenbuterol
|
tabs
|
150
|
€ 99.00
|
|
£ 70.71
|
£ 0.47
|
|
Clenbuterol
|
tab (20µg)
|
50
|
|
$50.00
|
£ 31.25
|
£ 0.63
|
|
Clenbuterol
|
tab (20µg)
|
200
|
|
$160.00
|
£ 100.00
|
£ 0.50
|
|
Clenbuterol
|
tab
|
50
|
|
$20.00
|
£ 12.50
|
£ 0.25
|
|
Pregnyl
|
amp (150µg)
|
1
|
|
$15.00
|
£ 9.38
|
£ 9.38
|
|
Pregnyl
|
amp (5mg)
|
1
|
|
$30.00
|
£ 18.75
|
£ 18.75
|
|
Primobolan
|
amp(50mg)
|
1
|
|
$21.39
|
£ 13.37
|
£ 13.37
|
|
Trenabol
(Trenbolone)
|
vial (750mg)
|
1
|
€ 119.00
|
|
£ 85.00
|
£ 85.00
|
|
Trenabol
(Trenbolone)
|
vial (750mg)
|
3
|
|
$320.00
|
£ 200.00
|
£ 66.67
|
|
Decabol
(nandrolone)
|
vial (250mg)
|
1
|
€ 115.00
|
|
£ 82.14
|
£ 82.14
|
|
Deca-Durabolin
|
vial (200mg)
|
1
|
€ 16.00
|
|
£ 11.43
|
£ 11.43
|
|
Deca-Durabolin
|
amp(50mg)
|
10
|
|
$160.00
|
£ 100.00
|
£ 10.00
|
|
Deca-Durabolin
|
amp (100mg)
|
14
|
|
$266.00
|
£ 166.25
|
£ 11.88
|
|
Deca-Durabolin
|
amp(50mg)
|
1
|
|
$9.00
|
£ 5.63
|
£ 5.63
|
|
Deca-Durabolin
|
amp (100mg)
|
1
|
|
$15.00
|
£ 9.38
|
£ 9.38
|
|
Deca-Durabolin
(BNF)
|
amp(50mg)
|
1
|
|
|
£ 3.54
|
£ 3.54
|
|
Tamoxifen
|
tab (20mg)
|
10
|
|
$32.00
|
£ 20.00
|
£ 2.00
|
|
Tamoxifen
|
tab (10mg)
|
10
|
|
$18.00
|
£ 11.25
|
£ 1.13
|
|
Tamoxifen
|
tab
|
30
|
|
$20.00
|
£ 12.50
|
£ 0.42
|
|
Proviron
|
tabs (25mg)
|
50
|
|
$39.00
|
£ 24.38
|
£ 0.49
|
|
Proviron
|
tabs (25mg)
|
10
|
|
$15.00
|
£ 9.38
|
£ 0.94
|
|
Proviron
|
tabs (25mg)
|
10
|
|
$15.95
|
£ 9.97
|
£ 1.00
|
|
Proviron
(mesterolone) BNF
|
tabs (25mg)
|
30
|
|
|
£ 4.75
|
£ 0.16
|
|
Trade Name and/or Drug
|
Preparation
|
Qty
|
Euros
|
Dollars
|
Sterling
|
Unit (£)
|
|
Omnadren
(Sustanon 250)
|
amp (250mg)
|
1
|
€ 11.00
|
|
£ 7.86
|
£ 7.86
|
|
Sten
(testosterone propio/cypionate)
|
amp (120mg)
|
2
|
|
$8.15
|
£ 5.09
|
£ 2.55
|
|
Sustanon
250
|
amp
|
50
|
€ 550.00
|
|
£ 392.86
|
£ 7.86
|
|
Sustanon
250
|
amp
|
30
|
|
$300.00
|
£ 187.50
|
£ 6.25
|
|
Sustanon
250
|
amp (250mg)
|
14
|
|
$238.00
|
£ 148.75
|
£ 10.63
|
|
Sustanon
250
|
amp (250mg)
|
1
|
|
$15.00
|
£ 9.38
|
£ 9.38
|
|
Sustanon
250
|
amp (250mg)
|
1
|
|
$16.85
|
£ 10.53
|
£ 10.53
|
|
Sustanon
250 BNF
|
amp (100mg)
|
1
|
|
|
£ 2.74
|
£ 2.74
|
|
Testabol
|
vial (1000mg)
|
4
|
|
$200.00
|
£ 125.00
|
£ 31.25
|
|
Testex
|
amp
|
15
|
€ 199.00
|
|
£ 142.14
|
£ 9.48
|
|
Testex/Testabol
Depot
|
vial (2000mg)
|
4
|
|
$225.00
|
£ 140.63
|
£ 35.16
|
|
Testosterone
Depot
|
amp (250mg)
|
30
|
€ 224.00
|
|
£ 160.00
|
£ 5.33
|
|
Testosterone
Depot
|
amp (250mg)
|
1
|
|
$8.00
|
£ 5.00
|
£ 5.00
|
|
Testosterone
enanthate
|
amp(250mg)
|
1
|
|
$11.55
|
£ 7.22
|
£ 7.22
|
|
Cetabon
(Stanozolol)
|
tab (2mg)
|
10
|
|
$13.00
|
£ 8.13
|
£ 0.81
|
|
Winstrol
|
tabs (5mg)
|
50
|
|
$35.00
|
£ 21.88
|
£ 0.44
|
|
Winstrol
(Stanozolol)
|
tabs (5mg)
|
200
|
|
$108.00
|
£ 67.50
|
£ 0.34
|
|
Menabol
(Stanozolol + Vit B)
|
tab (10mg)
|
1
|
|
$1.10
|
£ 0.69
|
£ 0.69
|
|
Stanabol
(stanozolol
|
tab (10mg)
|
150
|
€ 170.00
|
|
£ 121.43
|
£ 0.81
|
|
Stanabol
(stanozolol
|
tab (10mg)
|
200
|
|
$250.00
|
£ 156.25
|
£ 0.78
|
|
Winstrol
|
tab (20mg)
|
50
|
|
$250.00
|
£ 156.25
|
£ 3.13
|
|
Winstrol
|
tab (20mg)
|
1
|
|
$7.00
|
£ 4.38
|
£ 4.38
|
|
Stanabol
(stanozolol
|
tab (50mg)
|
100
|
|
$350.00
|
£ 218.75
|
£ 2.19
|
|
Winstrol
|
vial (50ml/10g)
|
1
|
|
$195.00
|
£ 121.88
|
£ 121.88
|
|
Winstrol
|
amp(50mg)
|
1
|
|
$15.00
|
£ 9.38
|
£ 9.38
|
|
Winstrol
Depot
|
amp
|
20
|
€ 227.00
|
|
£ 162.14
|
£ 8.11
|
4.4
From the above internet sources, the average prices
of different steroid preparations are as follows (Table
4).
|
Table
4 - Steroid Price Summary
|
|
Drug
|
Tab
|
Amp
|
Vial
|
|
Methanenedione
|
£0.53
|
n/a
|
n/a
|
|
Oxymetholone
|
£1.97
|
n/a
|
n/a
|
|
Boldenone
|
n/a
|
n/a
|
£78.13
|
|
Clenbuterol
|
£0.46
|
n/a
|
n/a
|
|
Nandrolone
|
n/a
|
£8.09
|
£46.79
|
|
HCG (Pregnyl)
|
n/a
|
£14.06
|
n/a
|
|
Mesterolone
|
£0.65
|
n/a
|
n/a
|
|
Stanozolol
|
£1.51*
|
£8.75
|
£121.88
|
|
Tamoxifen
|
£1.18
|
n/a
|
n/a
|
|
Testosterone
|
n/a
|
£7.07
|
£33.21
|
|
Trenbolone
|
n/a
|
n/a
|
£75.84
|
5.
Behavioural effects of Steroids
5.1
Animal Behavioural Studies: The effects of testosterone
on dominance and aggressive behaviour has been established
in numerous species of animals including primates Rejeski
et al[8]
showed increased aggressive behaviour in monkeys given
intramuscular injections of 4mg/kg testosterone propionate
(a.k.a. sustenon), including slapping, grabbing, stare
threat, chasing, fleeing etc. Joslyn[9] found
that female rhesus monkeys injected with 2mg testosterone
propionate 3x per week for 6 weeks increased aggressive
behaviour to such an extent that they replaced males
at the top of the social hierarchy. Rada et al[10] indicated
that social factors and learning influence the expression
of adult aggression.
5.2
Human behavioural studies: Susman et al[11] monitored the relationship between differences
in natural levels of steroids in adolescents and their
reported behaviour, finding those with higher levels
to be more sociable and outgoing, but more prone to
emotional sadness and other psychopathology. Udry et
al[12]
found serum testosterone levels to predict sexual motivation
and behaviour in early teenage boys, and Olweus et al[13] identified a significant association
between testosterone levels and self-reported verbal
and physical aggression, Ìlack of frustration tolerance",
and responsiveness to provocation and threat, but not
with antisocial behaviour or impulsiveness. Bahrke raises
the question as to the nature of this association, i.e.
to what extent aggressive behaviour per se may increase
levels of testosterone, rather than the reverse.
5.3
ÌNormal" Adult Males: Persky et al[14] found a correlation between testosterone
production rates and overall hostility among younger
men. Brown & Davis[15] report a significant correlation between
plasma testosterone and irritability, but noted expression
of aggressive behaviour to be highly dependent on other
factors and was absent in their 15 healthy college subjects.
Other researchers have questioned these results, either
finding weak positive relationships[16], or
no significant relationship[17] between aggressive behaviour and endogenous
testosterone levels.
5.4
In a controlled study using 20 healthy non-athletic
male volunteers with no prior history of steroid use,
Su et al[18] measured placebo baseline, low dose
methyltestosterone (40mg), high dose methyltestosterone
(240mg) and placebo withdrawal, and found the high dose
condition to produce significant increases in positive
mood (euphoria, energy, sexual arousal), negative mood
(irritability, mood swings, violent feelings & hostility)
and cognitive impairment (distractibility, forgetfulness
& confusion). One subject suffered an acute manic
episode with another subject becoming hypomanic. Previous
psychiatric history did not predict the reactions of
subjects.
5.5
Athletes & Bodybuilders: Studying bodybuilders
who were either current, past or non-users of steroids,
Lefavi et al[19] found that present users reported increased
anger-arousal and hostile outlook, while both present
and former users reported increased aggression, euphoria,
irritability and hyperactivity, the authors suggesting:
Ìpsychoactivity of anabolic steroids may be much greater
than previously believed"
5.6
In a retrospective study of 20 steroid users and 20
nonusers, Perry et al[20] reported users to show
significantly more depression, anxiety and hostility,
with symptom clusters including paranoid ideation (14
subjects - 70%) and psychotic features (13-65%).
5.7
Pope & Katz[21], in
a study of 41 bodybuilders and US Footballers using
10-100 times the medical doses of steroids (15mg-600mg
per day), found 12% reported Ìmajor" psychiatric
symptoms from Ìstacking" different preparations.
In a 1992 review[22],
the same authors considered the pattern of abuse and
withdrawal to be characterised by manic symptoms such
as irritability and euphoria, followed by depressive
symptoms[23] such as fatigue and suicidal tendencies
in withdrawal.
5.8
In 1994, Pope & Katz[24]
undertook a controlled study of 160 athletes, finding
23% of users to report major mood syndromes - including
mania, hypomania & major depression - associated
with periods of use, but were less likely to abuse other
drugs. They concluded that steroids in high doses may
cause serious mood disorders with substantial morbidity
for the user and victims of his irritability and aggression.
In a further study Choi & Pope[25] compared
23 steroid-using athletes with 14 nonuser athletes finding
users to report significantly more fights, verbal aggression
and violence towards their Ìsignificant other"
when using than between cycles (all but 3 users were
Ìstacking"). They considered steroids to increase
the levels of violence in those with pre-existing violent
tendencies, and to create a risk of violence in otherwise
nonviolent individuals. In March 1991, a UK magazine
article[26]
from a woman whose spouse had changed his personality
when using steroids, led to the formation of the Steroid
Users Wives Association.
5.9
In a critical 1994 review, Williamson & Young[27] considered thatÓ
Ìit is possible that people with a tendency towards violence
or a predispostion towards the development of a psychiatric
illness may me more likely to take anabolic-androgenic
steroids. It is also possible that, in susceptible individuals,
anabolic-androgenic steroids may induce psychological
changes or precipitate psychotic symptoms which could,
in turn, lead to violenceÓ
5.10
In a 1992 paper, Bahrke et al[28]
interviewed weightlifters divided into current (12)
previous(14) steroid users and nonusers (24). Current
and previous users repored increased enthusiasm, aggression,
irritability, insomnia, physical changes and changes
in libido, but found no significant dose-related effects,
and considered the effects to be either too subtle or
the assessment inventories insufficiently sensitive
to detect psychological changes. However, Bhasin &
Drew[29] reported
no evidence of increased violence among steroid-using
athletes - psychological tests and questioning of the
men's spouses found no evidence that steroids made them
angrier or more aggressive.
5.11
Prisoners: Kreuz & Rose[30]
first studied levels of testosterone and fighting, verbal
aggression and past criminal behaviour among 21 young
prisoners, finding those with adolescent records of
violent crime to have significantly higher testosterone
levels, suggesting testosterone to have an additional
effect on top of environmental and social factors increasing
the risk of, rather than creating, violent or criminal
behaviour.
5.12
Ehrenkrantz et al[31], in
an inadequately-controlled study, found significantly
higher levels of testosterone among prisoners classified
as Ìaggressive" and convicted of offences including
aggravated assault and murder, compared to nonviolent
offenders.
5.13
Rada et al[32] found a group of violent
rapists to have higher mean testosterone levels than
groups of child molesters, non-violent rapists or healthy
prison employees.
5.14
Schiavi et al[33] found
significantly increased testosterone levels among Ìviolent
delinquents" compared to nondelinquents and non-violent
delinquents, but no relationship between self-reported
measures of aggressivity.
5.15
Case histories involving anabolic-androgenic steroids
and violent crime: Pope & Katz[34]
described three men with no history of violence who
had committed violent impulsive crimes when taking steroids.
(a)
The first case was a prison officer with no history
of psychiatric disorder or violence, who had taken increasing
doses of a combination of steroids over 5 cycles, during
which he described himself as irritable and aggressive,
on a Ìhate the world" campaign, but with massively
increased self-confidence. During the fifth cycle driving
to work he was the butt of a mild joke at a local store
concerning a phone call, and returned later that day
in order to Ìscare the lady", forcing her into
his car, and shooting her when she tried to escape.
His identical twin brother, who also worked out with
weights but had never used steroids, showed no signs
of psychopathology.
(b)
The second case involved a 23 year old construction
worker who reported social drinking and occasional cocaine
use prior to using steroids. When using steroids he
reported severe mood changes, including Ìincredibly
shortened" temper, and Ìchallenging others for
no apparent reason". He became manic, irritable,
reckless and suffered delusions of grandeur ÌI was the
strongest person in the world, I was superhuman".
During his second cycle of steroid use, the man stopped
at a store and vandalised a payphone, later picking
up a hitchhiker to Ìhassle a little", drove him
to a remote woodland spot, and violently beat him up
without provocation, tying him between two polesm smashing
2x4 plank across his back, and kicking him, the victim
was later found dead. The attacker, following arrest
and withdrawal from steroids, reverted to his previous
mild-mannered personality with no subsequent indications
of violent tendencies. Although convicted of murder,
he escaped the death penalty as the judge considered
the steroid use to be a mitigating factor during sentencing.
(c)
The third case involved a 24yr old US football player,
having taken 12 courses of steroids since age 20. During
cycles he became more irritable at home, with family
and school, developing an attitude that he was the Ìbest"
and expecting special treatment from others, and was
assessed as Manic on DSM-III-R criteria, engaging in
reckless, dangerous and/or illegal behaviour. His fiancee
had broken off their engagement as he had been seeing
other women and, although at first indifferent, the
man became increasingly obsessed and discussed slandering
her, and eventually murdering his ex, stating he could
not get it out of his mind. He placed a homemade device
beneath her car and set it off as she left a party.
Although she was unharmed, he was arrested for attempted
murder. Following his arrest he developed a range major
depressive symptoms which cleared after four months.
Following conviction, the effects of steroids were taken
into account in determining sentence.
The authors considered the psychiatric symptoms as described
to be strikingly similar to those found in their 1988
study, with a stereotypic quality to the irritability,
aggressiveness and grandiosity experienced by steroid
users, and an obsessive escalation of responses to minor
insults, reinforcing their impression that
Ëthe symptoms and behaviour in the three men in our study
were primarily attributable to steroid ingestionÓ ÌOur
observations raise the possibility that anabolic steroids
may have contributed to many other violent crimes, but
that their role has gone unrecognised".
5.16
Lubell[35] reported the cases of
Horace Williams & Glenn Wollstrum (Pope & Katz
cases (b) & (a) above). In evidence in the Williams
case, Katz stated the defendant to be:
Ìsuffering the effects of anabolic steroids and had become
psychotic, unable to appreciate the wrongfulness of
his acts or the consequences of what he was doing."
5.17
In a single case report, Conacher et al[36]
cited the case history of a 32 year old Canadian bodybuilder
convicted or murdering his partner. He had been taking
steroids for 3 months before the incident, at about
6 times the medical dose (6x tablets dianabol per day
plus one ÌDeca" injection per week). Around a month
before the crime her reported becoming Ìhyper",
i.e. irritable, quarreling noisily, sleepless and increased
alcohol consumption. After a bout of heavy drinking
and discussing infidelities with his wife, he Ìsnapped"
and beat her severely such that she died of a subdural
haematoma. His changed mental state prior to the offence
were not related to steroid use at the time of his trial.
Following cessation of steroid use in prison, his mental
state reverted to normal.
5.18
Choi et al[37] noted prominent hostility
and aggression in subjective and objective ratings among
3 illicit steroid users compared with 3 comparable nonusers
in a longitudinal study over several months. One user
admitted an attempted murder during an earlier steroid
cycle.
5.19
Schulte et al[38] reported
a case of domestic violence associated with steroid
use, the 19 year old student & US football player
Ìstacked" intramuscular testosterone with oral
methandrostenolone over a 4 month period, increasing
his physical performance, but became increasingly irritable
and Ìrough" with his wife and 2 year-old son, whose
buttocks he scalded with boiling water in an attempt
at discipline. Two months following cessation of steroid
use the irritability and violent outbursts were resolved,
with no recurrence reported on 18 months follow-up.
5.20
Corrigan[39] reports two homicides
from Sydney, Australia, associated with steroid use,
also noting that by 1988 there had been over 20 such
cases reported in the USA[40].
(a)
Male bodybuilder, 29yrs battered wife to death with
claw-hammer while children were in the house, then shot
himself through the head. He had been using anabolic
steroids for several years, and was 7 weeks into a cycle
involving injections of stanozolol (sustanon) and testosterone
(organon), and was found to have a testosterone/epitestosterone
ration of 17:1, three times the ratio permitted in sports
testing (normal ratio 1:1). Corrigan considered there
to be little doubt that the behaviour fitted the features
of a steroid rage, as the home life was apparently happy
and he had not been known to be aggressive.
(b)
Male bodybuilder 22 yrs murdered a woman by repeatedly
bashing her head against a wall and kicking her, showed
no evident remorse and went home to bed. Had been on
8 week course of 50mg per week nandrolone (deca-durabolin,
organon), increased to 85mg (of a veterinary preparation)
for 3 weeks before the murder. He had never been known
to use other drugs, was from an apparently caring family
and had never been known to be violent. He had drunk
5-6 pints of beer in the 3 hours prior to the murder.
Corrigan considered this behaviour also to suggest a
steroid rage with the severe degree of violence and
indifference, albeit with the smallest dose of steroids
yet recorded for such a rage.
5.21
Oxymetholone, Methyltestosterone & Stimulants
Wilson et al[41] studied depressed men treated with tricyclic
antidepressants and methyltestosterone (oral 15mg/day),
and found that patients showed a paranoid response which
cleared when methyltestosterone was withdrawn. They
concluded that the paranoid reaction may arise from
an increase in aggression as a result of the combined
effect of the hormone (as MAO inhibitor) and increased
plasma monoamines (arising from imipramine), causing
additive effects on moodiness, paranoia and depression.
5.22
The study of Su et al[42] demonstrated
the effect of methyltestosterone on irritability, violent
feelings, hostility among other symptoms, and an acute
manic episode among one otherwise healthy volunteer.
5.23
Internet Ìuser guides": Oxymetholone (Anadrol,
Hemogenin,Anapolon 50, Oxitosona 50) is considered by
illicit users to be one of the strongest preparations
available in terms of anabolic effect and levels of
side effects[43]. One internet Ìuser guide"
quotes daily methyltestosterone dosages of 10-40mg per
day, with the highest rating for side effects, with
lower levels of efficacy than other preparations[44]. A Finnish internet steroid Ìuser guide"
quotes the following re methyltestosterone:
ÌMethyltestosterone is one of the oldest available oral
steroids. It is produced by many various manufacturers
and sold in a number of countries including the U.S..
It is quite androgenic, with minimal anabolic effects.
For athletic purposes, methyltest is generally only
used to stimulate aggression among power lifters and
those looking to boost up their workouts. Many methyltest
tabs are sublingual (to be placed under the tongue)
for faster absorption. These tabs can generally be identified
by a notable citrus flavor to them. A couple tabs placed
under the tongue before a visit to the gym may make
for an aggressive workout. Aside from this, methyltest
offers little except androgenic side effects. It is
quite toxic, elevating liver enzymes and causing acne,
gynocomastia, aggression and water retention quite easily.
Were one to tolerate these side-effects, methyltest
will offer little more than some slight strength gains.
One looking for quality muscle mass from a steroid cycle
should be looking elsewhere. Counterfeit steroids sometimes
contain only methyltest in an effort to deceive the
buyer. This is due to the fact that it is very cheap
in bulk and obviously may fool an inexperienced user."
5.24
Summary - steroids and violence The preponderance
of evidence from self-report and controlled studies
of steroids and behaviour, indicates a classical pattern
including the following symptoms.
|
Exaggerated
self-confidence
|
Irritability
|
|
Lack
of frustration tolerance
|
Excessive
response to provocation
|
|
Hostility
|
Mood
swings
|
|
Confusion/Forgetfulness
|
Distractibility
|
|
Libido
|
Paranoia
|
|
Violent
feelings
|
Mania
|
|
Violent
actions (verbal abuse and fights)
|
Serious
assaults with excessive violence
|
|
Reckless
as to consequences of actions
|
Obsessive
escalation of violence
|
5.25
Case studies and basic scientific research both point
to a particular danger of steroids used in combination
with stimulant drugs, whether antidepressants or illicit
stimulants. Both types of drug can cause unprovoked
or under-provoked aggression acting alone, in combination
their different modes of action would not only increase
brain catecholamine production, but would also inhibit
breakdown, causing a potential additive effect greater
than the sum of the two parts.
©
IDMU Ltd January 2004