Ecstasy
Consumption Patterns
Dosage (consumption)
and purity
The amount of MDMA and/or
related compounds in ecstasy tablets is extremely variable,
if indeed there is any contained at all. Independent
research[i]
has shown the tablets purchased may contain less than
1mg to 12mg. The Drugs Intelligence Lab[ii] have indicated that the average MDMA
content in tablets fell from 100mg in 1991 to 87mg in
1992. Saunders[iii]
after studying analyses of a number of different ¬Ecstasyÿ
tablets, has indicated that the doses of MDMA &
MDEA in tablets containing the drug range from 64mg
to 196mg, with most falling in the range 100-130mg.
There are a number of studies,
scientific, medical and sociological, which suggest
that the effective dose of MDMA is between 75mg and
100mg[iv]. Women, in general, require less to achieve
the same effect. By this token, one tablet should be
sufficient to produce the desired psychotropic effect
in a naive user. However, if the user takes tablets
of low purity, or containing other substances entirely[v] [vi]ingestion
of several tablets may not produce any discernible effect.
There is strong evidence
of development of an acute tolerance to the drug, as
with LSD, where repeated administrations have successively
diminishing psychotropic effects. Animal studies have
indicated decreased serotonin production, warning of
long-term neurotoxicity[vii],
and consequent tolerance over the longer term. It is
suggested that each person has 10 good trips"[viii]
before tolerance develops. This reduces the likelihood
of prolonged daily use, although prolonged binges"
may occur over a weekend with increasing doses used
on successive occasions.
Doses claimed to represent
up to 42 tablets have been reported as causing no detectable
long-term effects, although much smaller doses have
proven fatal. Risk factors include any person with a
tendency to high fever during childhood or adolescence.
The risk of toxic symptoms is not confined to the novice
user, as a successful experience in one instance can
be followed by a toxic episode using the same or even
a lower dose.
Most deaths attributed
to the drug have occurred at raves", and have been
due to severe overheating. The hot humid atmosphere
and high energy activity of a rave must be one of the
most dangerous places to take a drug which can cause
such increases in body temperature[ix].
High temperatures (over 43oC) have been reported as
causing minute blood clots to form, depleting the blood
of clotting factors, and paradoxically leading to internal
haemorrhaging. Some advice given to users to drink lots
of water may have led to recent tragedies outside the
hot ¬raveÿ environment, where the thirst induced by
the drug has led to death via cerebral oedema, or swelling
of the brain and internal organs.
The highest levels of use
over a single day are reported in the USA by Beck et
al[x] where respondents referred to
friends" who used 900mg in one sitting, plus a college
student who claimed to have used 1.25g (equivalent to
10-15 tablets) over a 24 hour period. A further long-term
user would binge" on a total of 1.5g (13-18 tablets)
over 24 hours. Both would binge over an evening or weekend.
The effective limit on bingeing would appear to be 2-3
days, after which a prolonged period of recuperation
would be required.
In the UK, ISDD[xi]
report weekend dosages of up to 20 tablets, and some
instances of chronic daily use of the drug over a 3
to 4 week period. The popular singer[xii] who claimed in an interview to use 12 tablets
per night would certainly fall among the minority of
heavier tolerant users, and would probably have suffered
neurotoxic damage as a consequence, and cause, of high
levels of ecstasy use.
Mixmag[xiii], in their 1999 survey of 1151
regular clubbers, found average number of tablets taken
per session was 2.82, with half having used 5 or more
tablets, one sixth having taken 10 or more, and 5% taking
15 or more. A quarter of respondents reported using
at least 4 tablets a night on a regular basis, a pattern
described by Winstock as ¬heavy chronic binge useÿ.
A further Mixmag survey[xiv] found 5.7% of respondents take between 9 and
22 pills at one session, with over 40% taking four or
more tablets.
Ecstasy consumption/purchase
data from IDMU 'Regular Users' surveys
Our 1994 survey[xv]
found that 14% of the drug users questioned used ecstasy
on a more or less weekly basis, with 3 percent doing
so more frequently. Occasional or experimental use was
the norm. Over 50% of respondents had never used the
drug. Regular users spent an average £88 per month on
the drug, equivalent to 5-11 tablets per month.
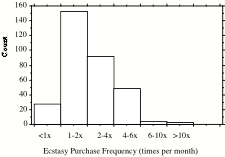
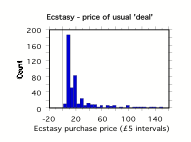
Our 1997 survey considered
the quantities purchased per occasion, and frequency
of ecstasy purchase. Ecstasy was most commonly purchased
in units of one to five tablets, with a small minority
of individuals buying ten or more tablets at a time.
The average price per deal was £28.08, equivalent to
3 tablets. Most users would purchase monthly, fortnightly
or weekly.
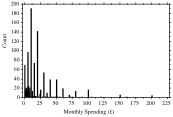
Fig 1. Ecstasy purchase
behaviour (1997/98)
Regular ecstasy users (weekly
or more often) in our 1997/8 surveys would spend an
average £41.33 per month (4-5 tabs) with a 95% upper
confidence limit of £147 per month (15-20 tabs). Regulars
would buy £37 worth per occasion (up to 5 tabs), with
a 95% upper confidence limit of £175 (20-30 tabs).
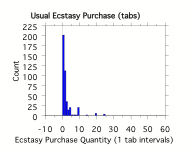
Data from our 2001-5 surveys
(total sample 9929, 3568 regular ecstasy users), suggest
that only around 1 in 10 regular ecstasy users consume
the drug on a daily basis (206 used during the week,
with 2276 respondents using at weekends). The average
number of tablets taken per day (daily users only) was
3.63, the average at weekends (all users) being 2.92
tabs per day.
Fig 2
Distribution of Daily Ecstasy Usage (2001-5)
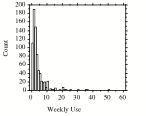
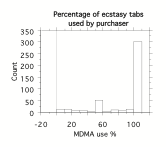
There were no significant
differences in the probability of supplying tablets
between experimental, occasional and regular users,
in each case an average of 80-90% of tablets were consumed
by the purchaser, representing 100% for the vast majority
of users.
Successive ¬Mixmagÿ surveys
have found that regular clubbers rarely purchase single
tablets at one time. In their 1999, 2000 and 2001[xvi] surveys, they found the average numbers of tablets bought on
each occasion for personal use were 8.16 , 8.92 and
12.0 tablets respectively, suggesting falls in prices
to result in an increase in the average quantity purchased
per occasion.
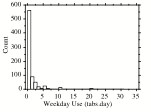
Although less than 10%
of regular ecstasy users used the drug during the week
24% of weekday users reported using 5 or more tablets
per day during the week, 58% used two or more tablets.
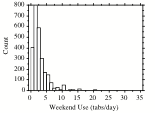
At weekends, 37% of users reported taking 3 or more
tablets, 17% took 5 or more tablets, 4% took 10 or more.
Overall 1% took 20 or more tablets per night, although
among weekday users this proportion rose to 4%.
|
Table
1 Ecstasy Usage (2001-5 IDMU surveys)
|
|
No of
|
Weekdays
|
Weekends
|
Weekly Total
|
|
tabs
|
n
|
%
|
Cum %
|
n
|
%
|
Cum %
|
n
|
%
|
Cum %
|
|
<1
|
1
|
0.5%
|
0.5%
|
33
|
1.4%
|
1.4%
|
111
|
15.1%
|
15.1%
|
|
1
|
86
|
41.7%
|
42.2%
|
789
|
34.7%
|
36.1%
|
187
|
25.4%
|
40.4%
|
|
1 < 3
|
48
|
23.3%
|
65.5%
|
597
|
26.2%
|
62.3%
|
152
|
20.6%
|
61.1%
|
|
3 < 5
|
21
|
10.2%
|
75.7%
|
473
|
20.8%
|
83.1%
|
130
|
17.6%
|
78.7%
|
|
5 < 10
|
31
|
15.0%
|
90.8%
|
283
|
12.4%
|
95.6%
|
105
|
14.2%
|
92.9%
|
|
10 < 15
|
11
|
5.3%
|
96.1%
|
69
|
3.0%
|
98.6%
|
27
|
3.7%
|
96.6%
|
|
15 < 20
|
0
|
0.0%
|
96.1%
|
15
|
0.7%
|
99.3%
|
8
|
1.1%
|
97.7%
|
|
20+
|
8
|
3.9%
|
100.0%
|
17
|
0.7%
|
100.0%
|
17
|
2.3%
|
100.0%
|
|
Total
|
206
|
100.0%
|
Av 3.63
|
2276
|
100%
|
Av 2.92
|
737
|
100%
|
Av 3.45
|
Effects of ecstasy
The main physiological
action is to increase the release of serotonin (5-hydroxy
tryptamine) and dopamine in the brain, changing the
mood of the user by altering the processing of information[xvii]. The half-life of ecstasy (MDMA) in blood is around 6 hours.
In general the effects are similar to, but more pronounced
than, those of Prozac or similar antidepressants which
block reuptake of serotonin thus raising the levels.
It could be said that they achieve the same effects
by ecstasy ¬turning on the tapsÿ, and Prozac ¬putting
in the plugÿ.
Physiological effects are
similar to other stimulants increased alertness and
physical energy, raised body temperature (in many cases
dangerously so), and dehydration. Liver and kidney damage
has been reported. Most deaths have occurred due to
overheating (heat stroke).
The main short-term psychological
effects are reported by Leister & Grob[xviii] as altered time perception
(90%), increased ability to interact with or be open
with others (85%), decreased defensiveness (80%), decreased
fear (65%), decreased sense of separation or alienation
(60%), changes in visual perception (55%), increased
awareness of emotions (50%), decreased aggression (50%),
speech changes (45%), awareness of unconscious memories
(40%), decreased obsessiveness (40% and cognitive changes
(40%)." Medium-term changes (up to a week) included
decreased sleep (40%), decreased appetite (30%), increased
sensitivity to emotions (25%), decreased ability or
desire to perform mental or physical tasks (20%), increased
ability to interact with or be open with others (20%),
and decreased defensiveness (20%)." Longer-term effects
(more than one week) included improved social-interpersonal
functioning (50%), changes in religious orientation
or practice (46%), changed values or life priorities
(45%), improved occupational functioning (40%), increased
ability to interact with or be open with others (35%),
decreased defensiveness (30%), changes in ego boundaries
(30%), decreased desire to use alcohol (25% )and decreased
fear (20%)" Other researchers have identified problems
with memory and judgement[xix], or increased sensitivity to
touch and sound[xx].
Short-term side effects
include dry mouth, clenching or grinding of teeth, reduced
appetite, weight loss, nystagmus, twitches, nausea and
cramp. Adverse effects on mood are attributed by Saunders
to the increased vulnerability of users when under the
influence, due to increased openness and reduced defensiveness,
such that insights may bring unbearable truths, and
candid disclosures may be regretted[xxi].
Adverse psychological effects include sleep disturbance[xxii], depression and paranoia[xxiii], and exhaustion after use[xxiv]. Tolerance to the effects of ecstasy develops
rapidly, such that the extreme euphoric effects tend
to be limited to the first few occasions of use, and
users may take increasing quantities in attempting to
achieve a desired level of intoxication. Regular users
can experience medium term depression[xxv]
when not under the influence, which tends to reinforce
ecstasy-seeking behaviour.
Evidence of damage to serotonergic
neurons[xxvi],
and lower serotonin levels among users and laboratory
animals, provides a physiological model predicting long-term
depressive illness in many chronic users. The neuronal
damage also explains why tolerance occurs, as no matter
how much stimulation they receive, the fewer remaining
neurons can only secrete a limited amount of serotonin.
Summary
Most recreational users
would use one to three tablets per occasion, regular
clubbers would typically use three to eight ecstasy
tablets per occasion[xxvii][xxviii]. However, there is a substantial minority
of ecstasy users who can consume 9-20 tablets over a
24-48 hour period[xxix][xxx].
© IDMU Ltd 2006